Using 3Shape TRIOS TO Scan Edentulous Patients - Dr. Lo Russo Interview
At the IDT International Digital Denture Symposium, Italy’s Dr. Lucio Lo Russo shook up the audience with his presentation on the design and production of dentures based entirely on TRIOS intraoral scans. A doctor attending the show, said that if there was one image that stuck in his mind during the two-day show, it was the photo documenting the incredible fit of one of Dr. Lo Russo’s dentures in a patient. We spoke with Dr. Lo Russo.
About Lucio Lo Russo
Lucio Lo Russo, DDS, PhD, is an Associate Professor of Oral Diseases at the School of Dentistry, University of Foggia, Italy. Prof. Lo Russo graduated from dental school in 1998 at the University “Federico II” of Naples (Italy), where he subsequently obtained his PhD. He is involved in basic and applied clinical research related to the diagnosis, treatment, and rehabilitation of oral diseases, in particular in the field of Oral Medicine, Periodontology, Operative and Digital Dentistry. He has published more than 140 scientific papers, most in high-impact international scientific dental and medical journals.
Until now, the innovation that has taken place with digital dentures has been on the lab side. With the ongoing development of software and materials, the digital design and production of removable dentures has progressed very rapidly, becoming almost, routine.
But on the clinical side, little has changed. We take an analog impression and that impression is then scanned to begin the digital workflow.
In my presentation at the IDT International Digital Denture Symposium, I demonstrated a new way to do digital dentures.
Accuracy of scanning dentures patients
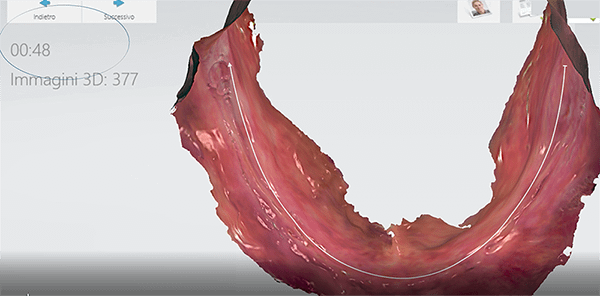
In my workflow, we begin with an intraoral scan of the edentulous patient. This caused quite a stir at the symposium.
Most people believe that it is not possible to begin the removable denture workflow with an intraoral scan. They believe that even if it is feasible, it is too difficult. Even worse, they think that an intraoral scan is not accurate enough to design dentures from.
Over the past three years, my colleagues and I have been doing research and demonstrated that concerns over the use of intraoral scans for removable dentures is in fact, not evidence based.
We have not had any problems capturing data using intraoral scans. Our work demonstrates and documents that intraoral scans are feasible and accurate enough for dentures, at least or as much so as conventional impression procedures.
Digital dentures made from intraoral scans require a different mindset. It’s like driving a car in the rain, it’s the same as driving a car in the sunny weather, it’s just different conditions.
I think we have been successful at it because we built our workflow on an evidence-based approach. I measured and tested every step of the way. We used trial and error and documented what worked. So instead of giving up, we just kept going.
You know when I first started trying to scan an edentulous arch, my mentor told me, okay you can try, but everybody says that it is not possible. It is not accurate.
But as we all know, intraoral scanners do capture gingiva and I felt if they could do that, then they can capture an edentulous arch, which is gingiva without teeth. Maybe it wasn’t the scanner at fault but the protocol.
500 digital dentures later
Now, nearly three years later, we have created more than 500 fully digital dentures. We start and finish the workflow without anything physical - a fully digital workflow for removable complete and partial dentures.
For professionals that are interested in learning more, all protocol steps are published in scientific journals.
The workflows are described point by point and can be found online.
The advantages of using an intraoral scanner
Basically, if you start your workflow with a digital impression instead of a conventional one, you have many advantages. For example, it is much more comfortable for the patient and you use less time.
If the patient has any type of gag reflex or allergy to impression material, the conventional impression procedure can become a very negative experience for the patient. On the other hand, with intraoral scans this is completely avoided and, most of the time, patients who have experienced conventional impressions, are favorably surprised.
Scanning an edentulous arch is much faster than waiting four minutes for conventional impression material to finally set. For us, on average, it takes about one minute to scan the edentulous maxilla and even less for the mandible. Of course, there can be variations from case to case or the patient. But on average it is much faster with an intraoral scan and more comfortable. In addition, you need fewer appointments. - See Dr. Lo Russo’s video of him TRIOS scanning an edentulous maxilla in 28 seconds.
If you compare it to a conventional workflow, you first need to make an intraoral scan to create the custom tray. Then with the custom tray you need to take the conventional impression and after, scan that. There’s really no reason to do all of this. We just start with the intraoral scan of the edentulous arch.
On top of saving time, there’s no need to ship the impression or cast to a lab, so I save time and money. Basically, every step in the conventional workflow requires additional time, additional material, additional costs and most important, adds a potential source of error. With analog, we lose standardization and we can lose accuracy when we arrive at the final denture.
As I mentioned earlier, with digital, we have documented that we end up with a denture that is at least, or as accurate as a conventional impression.
Lastly, aside from the wear and tear that can result in sending a conventional impression or physical casts back and forth, another important aspect to consider is safety. All this contact with the patient’s mouth is theoretically, potentially infected. So, if we are not transferring anything from the clinic to the lab, we are reducing and controlling, any chance of infection.
As our papers document, there is really no reason to not start the removable denture workflow with an intraoral scan.
Why 3Shape TRIOS?
That’s easy, the reason we did our research using TRIOS was practical, we owned a TRIOS. But to be honest, I have yet to see any validated scans from the other intraoral scanner-makers of edentulous arches like I have done with TRIOS.